FENS liveblog
 I’m currently in Dublin, attending the European Nutrition Conference (FENS), and will try to provide some updates during the week. The conference starts tomorrow, Tuesday October 15, and last until friday.
I’m currently in Dublin, attending the European Nutrition Conference (FENS), and will try to provide some updates during the week. The conference starts tomorrow, Tuesday October 15, and last until friday.
You can find my conference notes here, including the abstracts of the talks I’ve attended. Also, and you can find updates by following #FENS2019 on Twitter!
Tuesday - Day 1
 It’s 09:45 and dhe conference is about to start, with the opening ceremony followed by the first plenary session. 1700 participants from all over the world are getting ready for a week of nutrition research, discussions and networking!
It’s 09:45 and dhe conference is about to start, with the opening ceremony followed by the first plenary session. 1700 participants from all over the world are getting ready for a week of nutrition research, discussions and networking!
Malnutrition in an obese world
The first plenary lecture was presented by Joäo Breda, from the World Health Organization, on the topic of Drivers across the lifecycle of malnutrition in an obese world - European perspectives. His talk focused on the importance of nutrition in reaching many of the sustainable development goals. Using data from European countries, he illustrated nutritional challenges such as the increasing prevalence of childhood overweight and obesity. The first pillar in the European Food and Nutrition Action plan 2015-2020 is to create a healthy food and drink environment. This include strategies to reduce the intake of sugar and salt. The second pillar is nutrition during life cycle, where Breda was not happy with the low compliance to exclusive breast feeding in the European countries. The rest of the talk focused on the final three pillars, including the large potential for improving the communication of nutritional information to the public, as well as the need for improving nutritional surveilance and research regarding the implementation of selected interventions.
Genetics, salt, riboflavin and hypertension
The next session I attended had 3 speakers. First, Catherine Graham told us about The associations between genetics, salt taste perception and salt intake in young adults. Salt intake continues to be the #1 dietary risk factor for non-communicable diseases, but reducing salt intake is difficult. A preference to salty taste, as well as genetic factor lowering the salt taste sensitivity, may be contributors to the persistent high salt intake in populations.
Next up, Martina Rooney told us about Central blood pressure in adults screened for a genetic polymorphism in folate metabolism. Genes are commonly regarded as non-modifiable risk factors, but in the presence of high-penetrance gene-nutrient interactions, this paradigm does not necessarily hold. A genetic variant in the MTHFR gene (C677T), affecting ~10% of the population, has been consistently linked to hypertension risk, and this variant is responsive to low-dose riboflavin supplementation. Previous research have focused on preipheral blood pressure. In her research, Rooney have shown that these individuals also have higher central blood pressure.
Finally, Emma O’Sullivan continued the MTHFR TT-story, by investigating riboflavin status in a population screened for this genotype. They found no large differences in riboflavin status or intake across the MTHFR genotypes, but a large proportion (14% of men, 22% of women) of the population have intakes below the EAR. How riboflavin status affects the blood pressure in the population should be further addressed.
Metabolic obesity
After lunch I attended the session on metabolic obesity. Overweight and obesity is commonly classified by BMI, but this doesn’t tell us much regarding metabolic health.
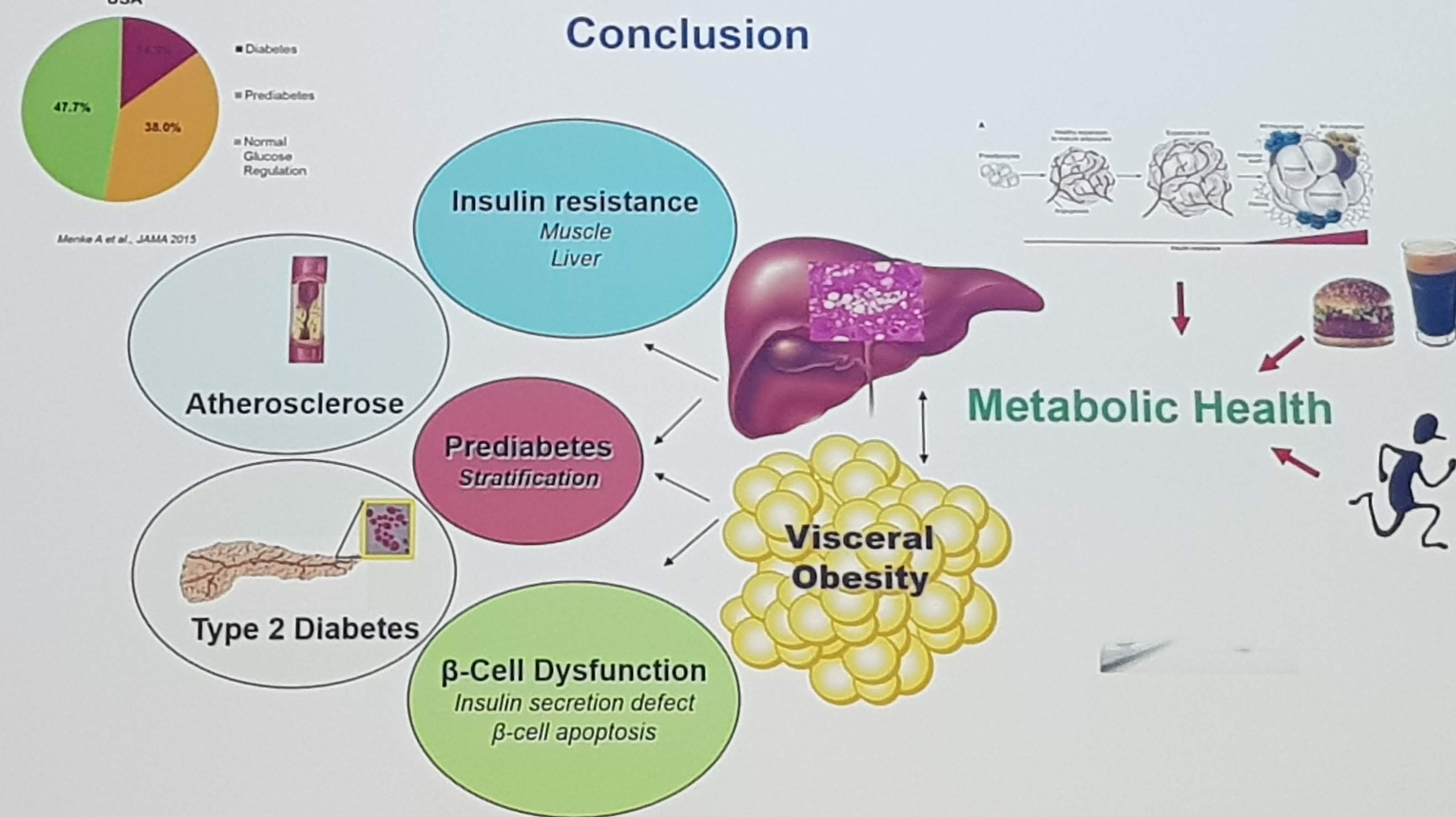
The first talk was by Norbert Stefan, on Definition and clinical Impact of metabolically healthy and unhealthy Obesity. Although obesity is a key risk factor for life style diseases, the risk is only moderately elevated in those with a metabolically healthy phenotype. At the same time, normal weight people with a metabolically unhealthy phenotype also have increased mortality. A strong correlation have been reported between liver fat and insulin resistance, which is stronger than the association with visceral fat mass. The concept of metabolically healthy obesity was presented, and defined by being obese but having < 2 metabolic risk parameters, and data was presented suggesting that about 25% of obese persons were metabolically healthy. Further, compared to metabolically healthy normal-weight, being metabolically healthy obese was associated with only 28% increased risk, while the metabolically unhealthy normal-weight had 115% increased risk. In conclusion, he recommend to stratify the risk assessment according to metabolic health to accomplish the goal of providing personalized treatment to patients.
Louise Thomas then told us about current advances in our methods of predicting visceral fat mass. Common methods are MRI scans and DEXA. Thomas showed that these methods are actually measuring different things, but as they are highly correlated, this suggests that this is a scaling issue. A proxy measure is based on waist circumference, which works well on the group level, but is less good on the individual level. MRI continues to be the gold standard, but simpler methods such as predictive algorithms shows promise, especially combined with machine learning.
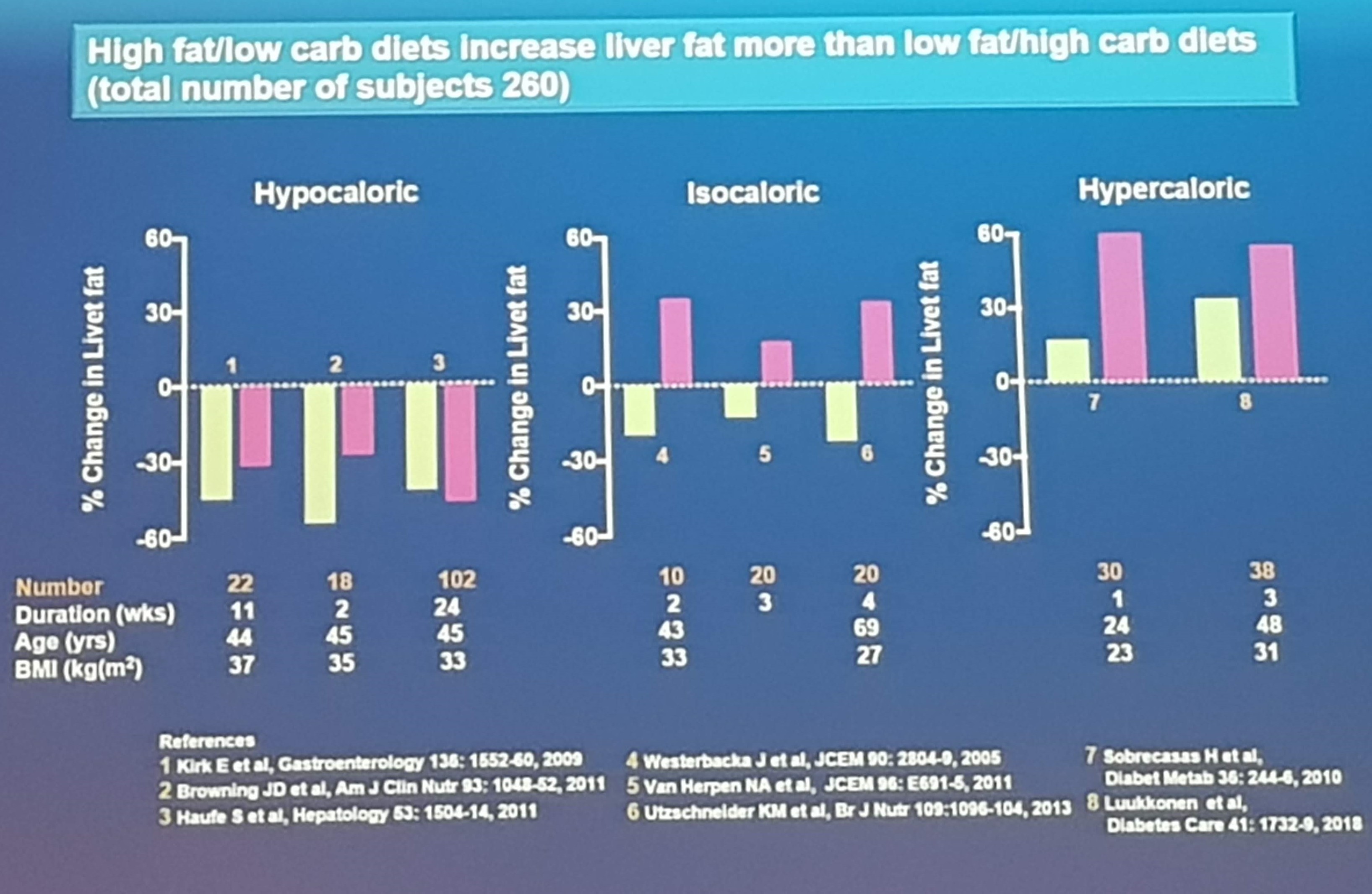
To close the session, Hannele Yki-Järvinen presented on the Effects of overfeeding different diets on the human liver, with a focus on the accumulation of liver fat. She showed data that metabolically determined non-alcoholic fatty liver disease (NAFLD) is dominated by saturated triglycerides and ceramides, and increases the risk of insulin resistance. On the other hand, genetically determined NAFLD is dominated by polyunsaturated triglycerides, and does not increase insulin resistance risk. When considering the effect on dietary composition on liver fat, several smaller studies have shown that low-carb/high-fat diets increases liver fat more than the high-carb/low-fat diets.
Further, saturated fat increases liver fat more than polyunsaturated fat.
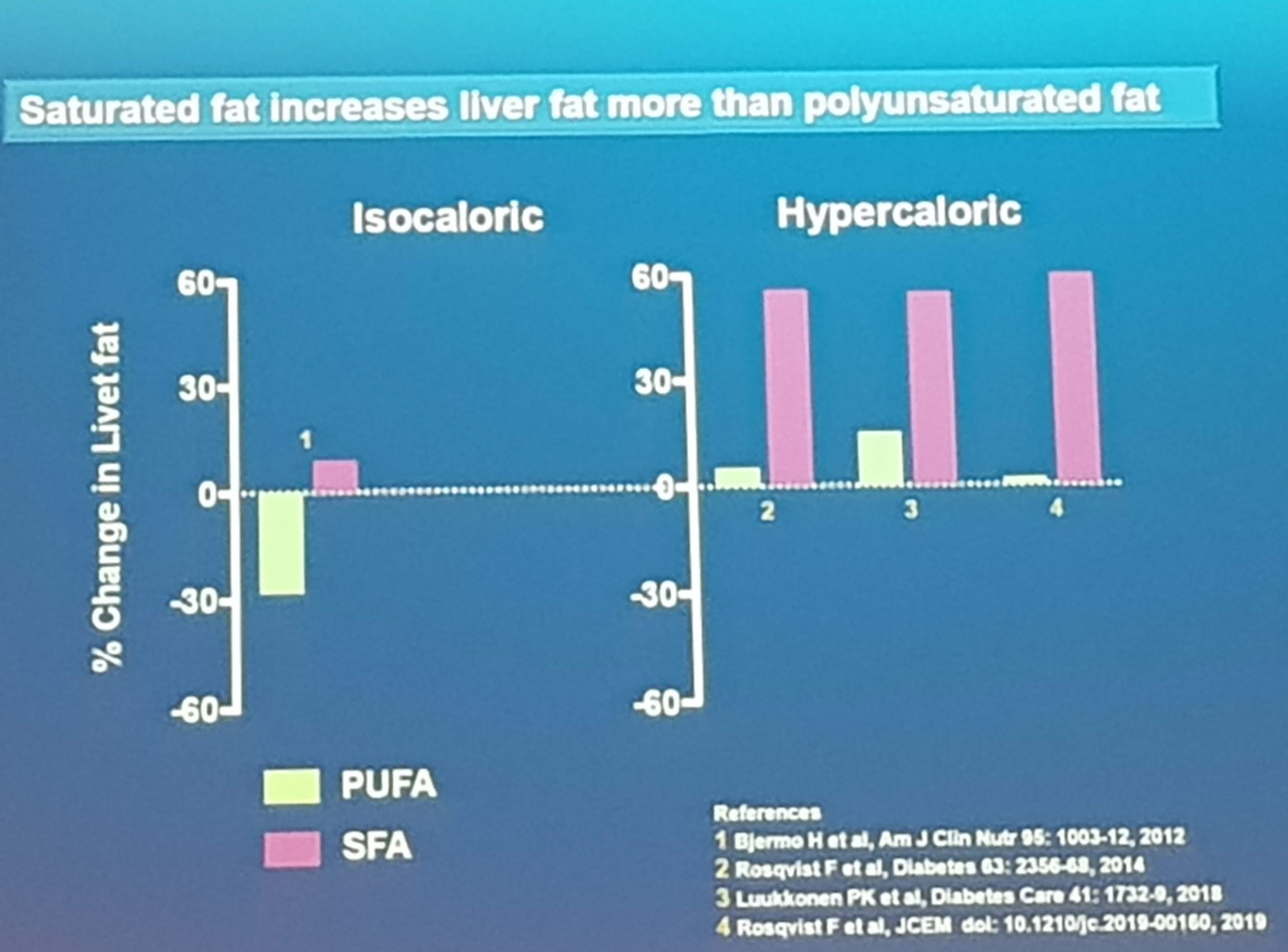 Metabolically determined NAFLD can be a consequence of overeating simple sugars, due to increased de novo lipogenesis. However, in the context of similar weight gain, saturated fat induces greater metabolic harm compared to simple sugars.
Metabolically determined NAFLD can be a consequence of overeating simple sugars, due to increased de novo lipogenesis. However, in the context of similar weight gain, saturated fat induces greater metabolic harm compared to simple sugars.
Nutrition communication
In the next workshop, the topic of communication of nutrition information was on the agenda. This is a big challenge as nutrition information is now available from numerous sources including the media, internet, health professionals, social influencers and peers.
The first talk of the workshow was given by Robert O’Connor, asking the question What’s driving the nutritional problem in cancer?. In his talk, he focused on the multitude of dietary recommendations aimed at cancer patients, and their challenge in discerning between evidence-based and pseudoscientific information. A problem he referred to as “scientification” of nutrition advertisement. One increasingly popular phrase in food advertisement is “let food be thy medicine”, on which O’Connors comment was “food is not medicine for healthy people, it simply isn’t”. He discussed the problems of health “shockumentaries” spreading misinformation, and further pointed out that although science is increasingly available, scientific understanding is not. The finishing point was that the impact of this confusing terrain of misinformation is an increase in preventable cancer mortalities due to people following unfounded advice, including postponing or not receiving actually evidence-based treatments.
In the next talk, Eileen O’Sullivan, cancer patient and patient advocate, talked about what advice the public believes. As a patient, she did not receive any specific dietary advice from the hospital, but met many “snakeoil salesmen”, trying to take advantage of her vulnerability as a patient. She raised the point that not only patients themselves, but also relatives, are targeted by people offering non-evidence based advice. And this advice doesn’t only come from amateurs, there are many examples of doctors and nutritionists giving harmful advice. Phrases such as “This food feeds your cancer”, “Big pharma wants you to be sick”, and victim blaming such as “you are sick because you ate this and that”, are not uncommonly encountered for a cancer patient. Ketogenic diets, alkaline diets, raw food, functional food, paleo diet, fasting and organic are only some examples of pseudoscientific dietary fads targeting cancer patients. There is an increased need for nutritional professionals to counter this misinformation and provide evidence-based advice.
Journalist and radio-presenter Philip Boucher-Hayes then provided his thought on Journalism and the proliferation of nutribabble. He started by pointing out that noone sells books or TV programs with boring advice such as eating a little bit less or moving a little bit more. And when writing his book, he discovered that there really were no fact checks, and that correctness was prioritized below novelty. The same goes for TV-shows, which he describes as less fact checked than the commercials between the shows. He finished his talk by encouraging researchers to occupy the same space as the charlatans does, and to do this by talking in a language people can relate to, not “like an academic”, as well as keeping the message brief and to the point.
To finish the workshop, Gabriel Scally gave a talk on Full disclosure - on food and nutrition. He started by disagreeing with the notion that science is highly accessible, referring to the problems of paywalls limiting the access to the majority of scientific publications. And without confirming or denying it’s helpfullness of resources such as Sci-hub, let’s just say it was mentioned. He then continued by talking about content of food that is not disclosed, such as pesticide and antibiotic residue. He did emphasize that the doses are small, but his position was that it should be disclosed.
Low-carbohydrate diets and diabetes
The final talk I attended on the tuesday was by Chaitong Churuangsuk, who performed a systematic review of reviews of the effectiveness of low-carbohydrate diets. Overall, his analyses of 10 systematic reviews suggested that the difference in weight loss compared to low-fat diets were small (< 1 kg). However, he observed that reviews of lower quality, as well as the reviews reporting larger effects, were more frequently cited. He further observed that potential risk of nutritional deficiencies, such as iodine, was being neglected in the literature. Churuangsuk concluded that low-carbohydrate diets could be effective for weight loss, and also may lower HbA1c and the need for diabetes medications, especially when weight loss was achieved. However, long-term safety, and potential negative effects including increased LDL-cholesterol should be considered. The latter can be mitigated by designing a low-carbohydrate diet with plant based protein and fat sources, limited in saturated fat.
Wednesday - Day 2
Day 2 of the conference is about to start, with a keynote lecture from Arne Astrup. Later today my plan is to attend some sessions on personalized nutrition, and at the end there will be a debate on whether the individual or the society have the primary responsibility to prevent obesity.
Weight management according to glucose metabolism
Arne Astrup presented the first keynote on Personalized dietary obesity weight management determined by glucose metabolism and microbiota. In his talk, he showed data from weight loss trials, demonstrating highly variable results. Based on research suggesting that carbohydrates may have a great satiating effect in insulin sensitive individuals, but maybe less so in those with insulin resistance, he provided the hypothesis that those with prediabetes and diabetes would benefit from a lower carbohydrate diet. By reanalyzing data from large international diet studies, such as this one, they have shown that insulin resistant individuals with diabetes or prediabetes responds better to lower-carbohydrate and high fiber diets, when considering weight loss and maintenance. In the second part of his talk, he showed data suggesting that gut microbiota also contributes to the individual response to dietary exposures. In particular, the effect of fiber seems dependent on the microbiota composition. In conclusion, Astrup holds the position that we should start providing individualized recommendations for weight management based on glycemic status, while the data on microbiota, albeit promising, needs more work. During the question session, he emphasized that he recommended a moderate carbohydrate restriction, and that he was not a big fan of very restrictive diets.
Nutrigenomics, are we there yet?
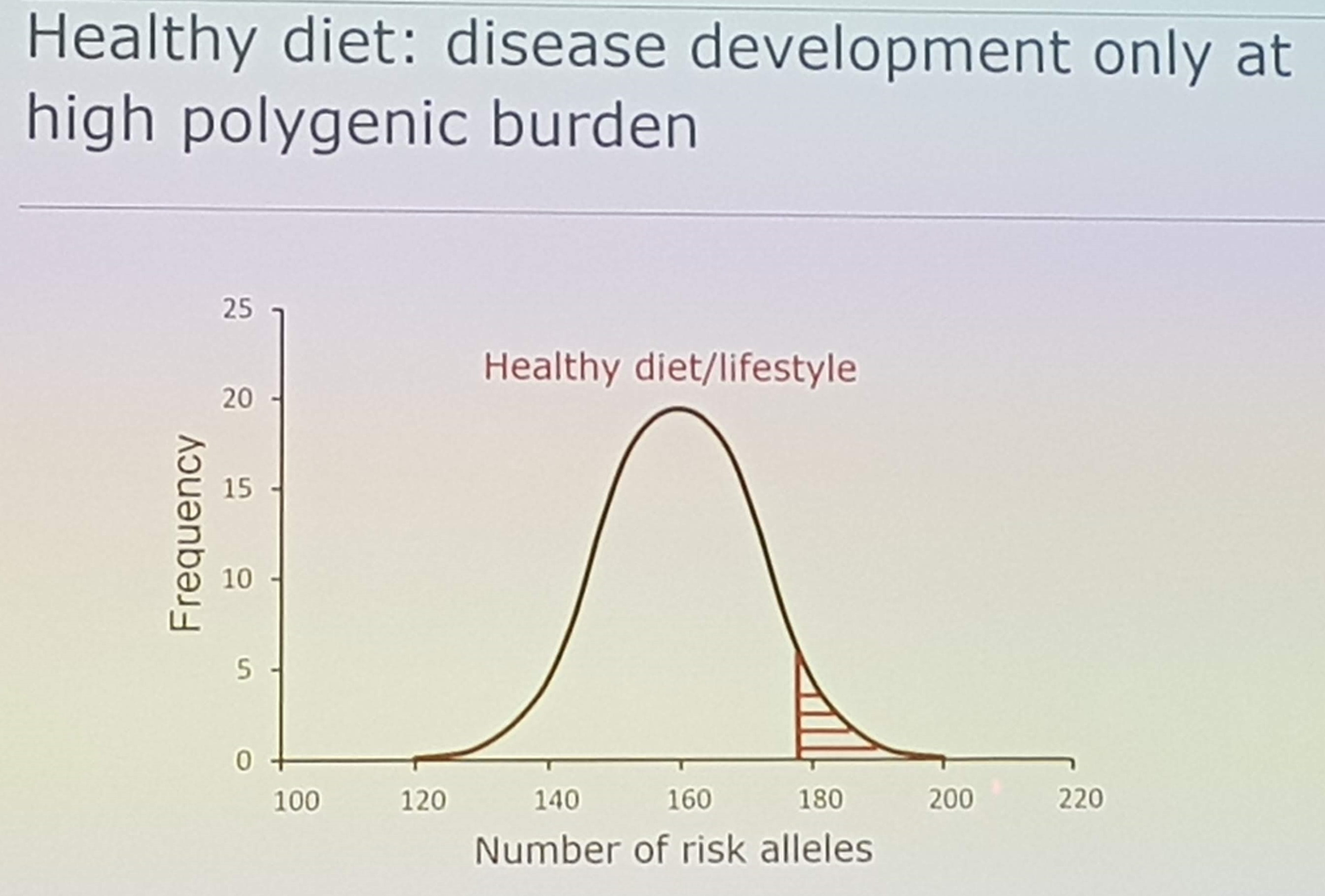
In the next session I attended, the topic was nutrigenomics. In the first talk, Sander Kersten started by telling us about gene-nutrient interactions, that work both ways. Nutrigenomics refer to how the food influences our gene expression, while nutrigenetics refer to how our genes influence our response to diet. For polygenic diseases, we all carry on average 160 risk alleles. By following a healthy diet, achieved by general or personalized recommendations, you can delay or prevent disease development relative to your polygenic burden.
 However, risk cannot be monitored on the individual level, but biomarkers can. In the future, with improved technology including wearables etc, nutrigenomics can contribute to identify individuals for early dietary interventions. Kersten closed his lecture by pointing out that there’s still a large knowledge gap, especially in providing mechanistic explanations for well established effects such as the triglyceride lowering by omega-3 fatty acids, or the cholesterol raising effects of trans fatty acids of cafestol. Nutrigenomics can contribute to fill this gap.
However, risk cannot be monitored on the individual level, but biomarkers can. In the future, with improved technology including wearables etc, nutrigenomics can contribute to identify individuals for early dietary interventions. Kersten closed his lecture by pointing out that there’s still a large knowledge gap, especially in providing mechanistic explanations for well established effects such as the triglyceride lowering by omega-3 fatty acids, or the cholesterol raising effects of trans fatty acids of cafestol. Nutrigenomics can contribute to fill this gap.
Stephen O’Rahilly was supposed to give a talk on The causes and consequences of obesity, but decided to go off script and focus on growth differentiation factor 15 (GDF15). GDF15 is a hormone signalling to the brain in situations of stress, and facilitate aversion towards that stimuli. Providing GDF15 to animals have been used to induce aversion towards certain foods. Circulating amounts of GDF15 is not postprandially regulated, but chronic nutrition stress such as overfeeding increases the concentrations. Also, animals lacking GDF15 are more likely to become obese, and weight loss obtained by metformin treatment is highly correlated to the degree of increase in circulating GDF15. Collectively, this suggests a role in body weight regulation. Further, a role of GDF15 in cancer cachexia and in hyperemesis gravidarum was discussed, providing a potential future target for treatment.
The last talk of the session was given by Hannelore Daniel, on the topic of Nutritional phenotyping, which she defined as “assessing and quantifying the acute and chronic resonses of the organism to the individual food items or diet”. During the day, we constantly switch between anabolic and catabolic state, and a relevant question is whether the anabolic/catabolic space is different between people. She presented data from the HuMet and nutriTECH studies, where participants were exposed to different interventions and extensively phenotyped. They were able to identify different metabotypes who presented different responses to metabolic challenges such as weight loss. This suggests that phenotyping may be helpful to predict effects of nutritional interventions.
Personalized nutrition for health
After lunch I attended the symposia on personalized nutrition for health, with the outspoken goal of seeking to “address the hype versus hope, fact versus fallacy, that is anticipated from Personalised Nutrition research and to understand whether the Personalised Nutrition paradigm is relevant to all health/age contexts”.
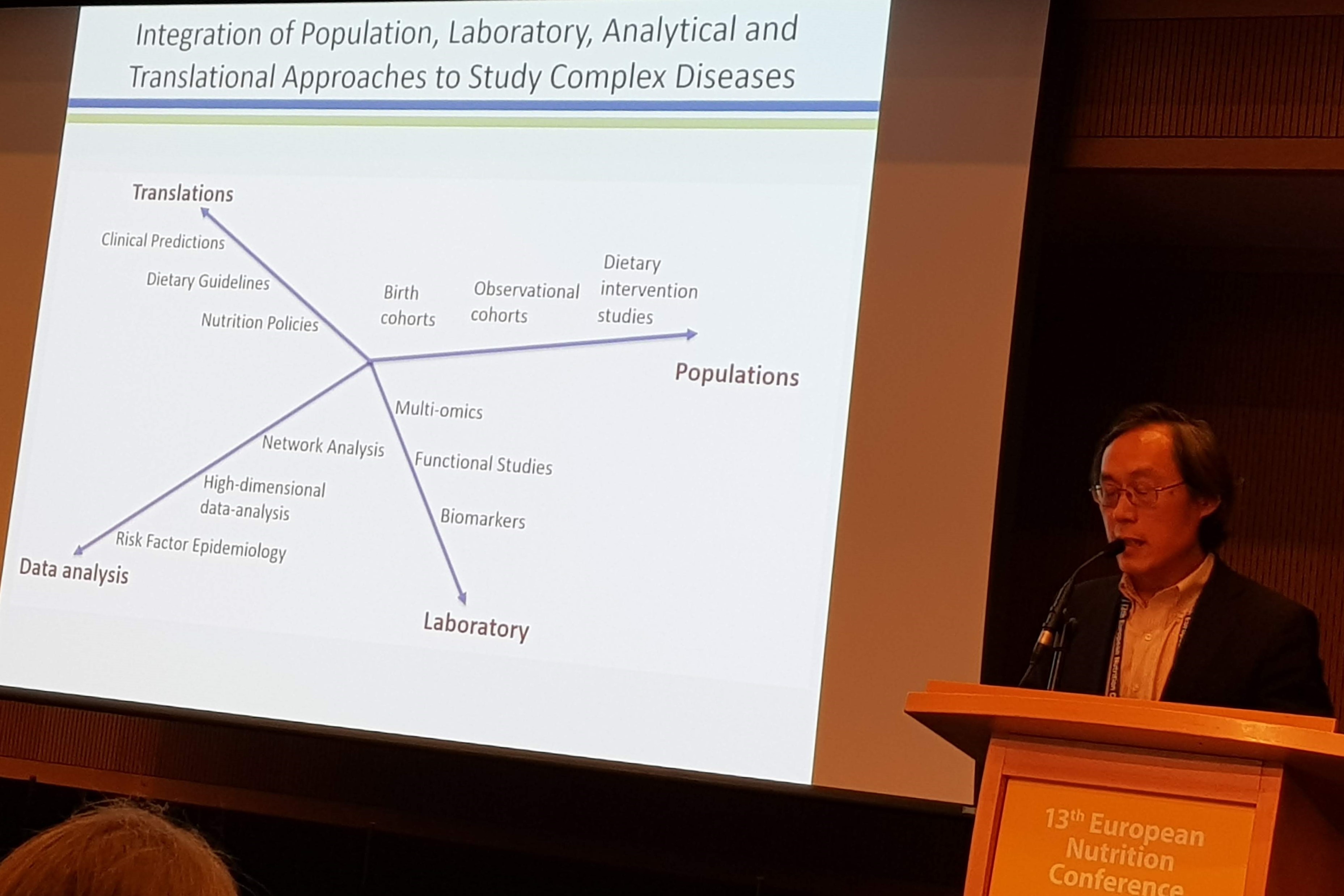
The first speaker was Frank Hu, who talked about Precision nutrition for the prevention and management of cardiometabolic diseases: Hype or hope?. He started by saying that modern nutrition research needs to integrate different approaches to make progress.
 According to Hu, the goals of precision nutrition are wider than just providing recommendations to the individual. It also includes improving out ability to measure diet accurately. In a recent study they compared different dietary instruments, and concluded that a 2 week food record was the most accurate method. However, when compared to biomarkers, a food frequency questionnaire performed as well as a 7-day food record. Hu continued the talk by showing data from PREDIMED, where they developed a metabolic signature capturing the adherence to the mediterranean diet. This signature was more strongly related to CVD risk than self-reported adherence, suggesting a role for metabolic signatures as measures of dietary adherence.
According to Hu, the goals of precision nutrition are wider than just providing recommendations to the individual. It also includes improving out ability to measure diet accurately. In a recent study they compared different dietary instruments, and concluded that a 2 week food record was the most accurate method. However, when compared to biomarkers, a food frequency questionnaire performed as well as a 7-day food record. Hu continued the talk by showing data from PREDIMED, where they developed a metabolic signature capturing the adherence to the mediterranean diet. This signature was more strongly related to CVD risk than self-reported adherence, suggesting a role for metabolic signatures as measures of dietary adherence.
Of course Hu also touched upon the recent publication on red meat intake, concluding that the evidence, albeit extremely consistent, was weak and that we should just continue our current intake. Hu pointed out that the criteria used by the authors are not suited to assess the level of evidence in epidemiological research, and that applying the same criteria to any lifestyle-disease association would come to the same conclusion, also for well established risk factors as physical inactivity, secondhand smoking etc.
Hu mentioned a few examples of commercially available test kits such as Day Two and 23andme, who offer personalized nutritional advice based on your microbiome or genetics. However, he pointed out that the science behind these advice is simply not there, questioning their usefulness. Hu finished his talk by emphasizing that obesity is not driven by changes in our genes, but by changes in our food environment. Therefore personalized nutrition must be integrated with public health nutrition as well as planetary nutrition, to promote personal, personal and planetary health.
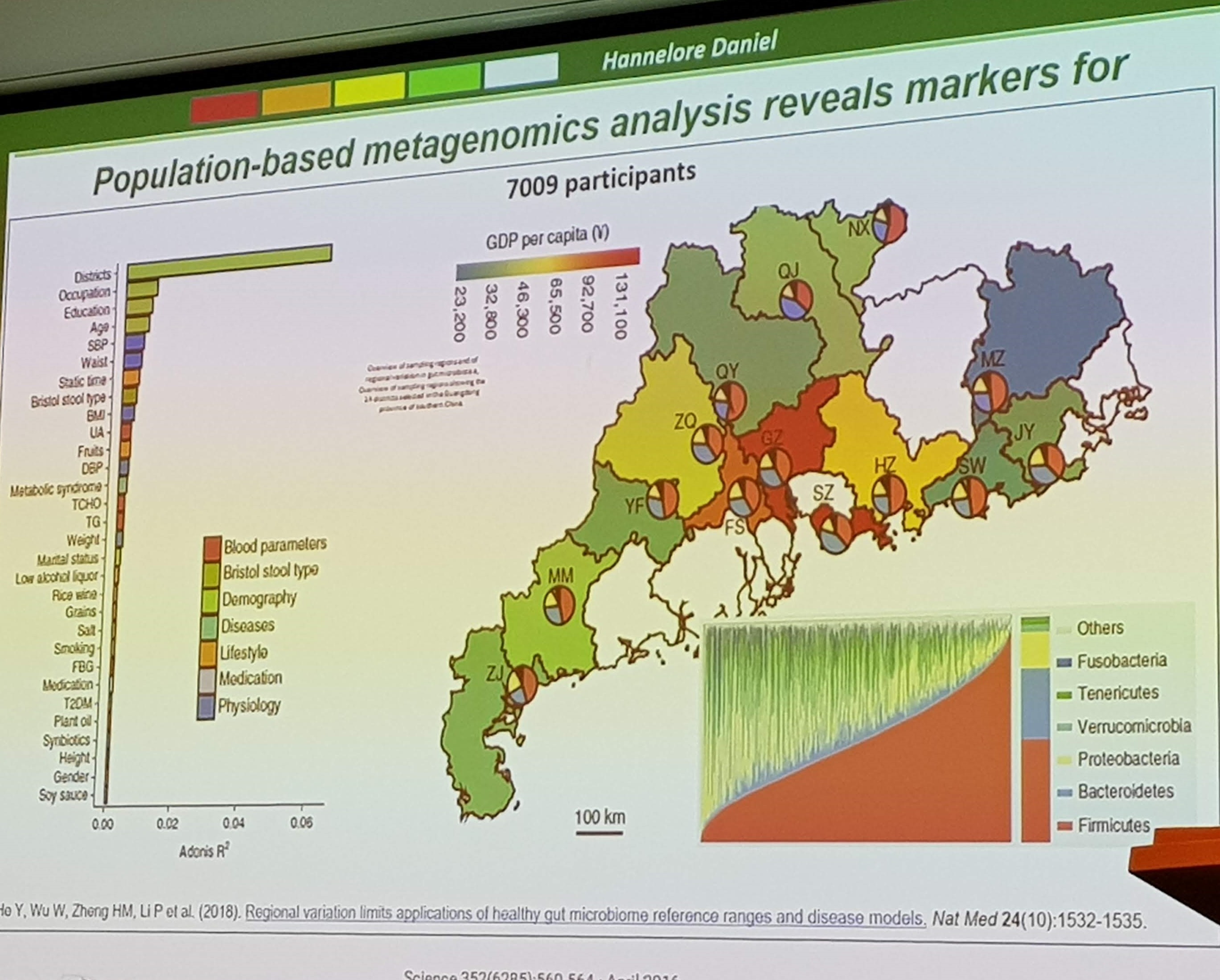
The next speaker was Hannelore Daniel, with her talk titled Personalised nutrition for the metagenome: host versus microbiome. She pointed out that although diet influences the microbiome, geographical location was by far the most important factor. And therefore, diet-microbiome effects are hard to replicate in different contexts.
 For many years we have believed that we are vastly outnumbered by our bacteria, but Daniel points out that this number traces back to a single publication from 1972, which has never been questioned. More recent analyses conclude that the bacteria content in our intestines comprises ~95g, and cell count to be approximately 1:1 with human cells. The main take-home point from this talk was that we should not forget gastrointestinal physiology when attributing health effects to the microbiome. Altering intestinal transit time have a profound effect on microbial amount and diversity, and has also been shown to influence health related parameters.
For many years we have believed that we are vastly outnumbered by our bacteria, but Daniel points out that this number traces back to a single publication from 1972, which has never been questioned. More recent analyses conclude that the bacteria content in our intestines comprises ~95g, and cell count to be approximately 1:1 with human cells. The main take-home point from this talk was that we should not forget gastrointestinal physiology when attributing health effects to the microbiome. Altering intestinal transit time have a profound effect on microbial amount and diversity, and has also been shown to influence health related parameters.
The last talk of the session was given by Lorraine Brennan, on the potential of Precision Nutrition to improve Health. When talking about precision nutrition, Brennan refer to the concept of giving specific advice to the individual, which is different from what we do today where we give different advice to specific subgroups. In a study where participants received either standard advice, or personalized advice based on blood and gene tests, higher adherence was observed in the latter group, demonstrating the potential for this approach. In the next part of the talk was considering using biomarkers as a complement to self-reported dietary intake data. Brennan used proline betaine as an example of a biomarker of citrus intake. Recently, they published a paper on combining biomarker data with self-reported data to correct for misreporting, which is a promising approach to improve dietary intake data. Brennan finished her talk by telling us about her approach for developing targeted recommendations to segments of the population, through metabotyping and decision threes.
Low-calorie sweeteners
After the session on precision nutrition, I moved on to a session on the use of low-calorie sweeteners. First up, Margaret Ashwell presented the Report from a 2018 Expert Consensus Workshop on recommendations about the use of low calorie sweeteners. Different views prevail, where although everyone agrees that sugar intake should be reduced, people disagree whether low-calorie sweeteners are a good alternative. The report considered three main topics, namely weight management and glucose control, safety and consumer perception and the role of sweeteners in relation to policy. They report on what is known, what is not known and what should be done. The panel agreed that low-calorie sweeteners are safe, and can help reducing sugar intake. They conclude that the sweeteners have the same effect on appetite as water. Further, the negative effects reported in relation to cardiometabolic health is most likely due to confounding by adiposity. However, less is known about long-term effects, what is driving the different consumer perception, and how low-calorie sweeteners influence diet quality in the longer term.
Anne Raben continued the session by presenting results from trials and metaanalyses of low-calorie sweeteners on parameters of body weight and glycemic control. Overall, compared to sucrose, the low-calorie sweeteners was associated with reduced body weight. In one study, low-calorie sweetener was even superior to water, which potentially can be explained by the fact that having a sweet option may increase adherence to the diet as compared to just having water. Several studies have also considered the effect on glycemic control, and consistently conclude that the sweeteners are beneficial when compared with sucrose.
The last talk of the session was given by Jason Halford, presenting his research on the consumer’s views. He showed results indicating that most low-calorie sweetener consumers report that they enjoy them, and also use them as a tool for body weight control. Interestingly, in a recent paper they found that low-calorie beverage consumers actively seeked these beverages in situations of craving, and did not overconsume calories. Sugar-sweeteened beverage consumers, on the other hand, were more likely to overconsume when exposed to cravings. This indicates that low-energy sweeteners can be a tool to handle cravings to avoid overeating.
Biomarkers of riboflavin status
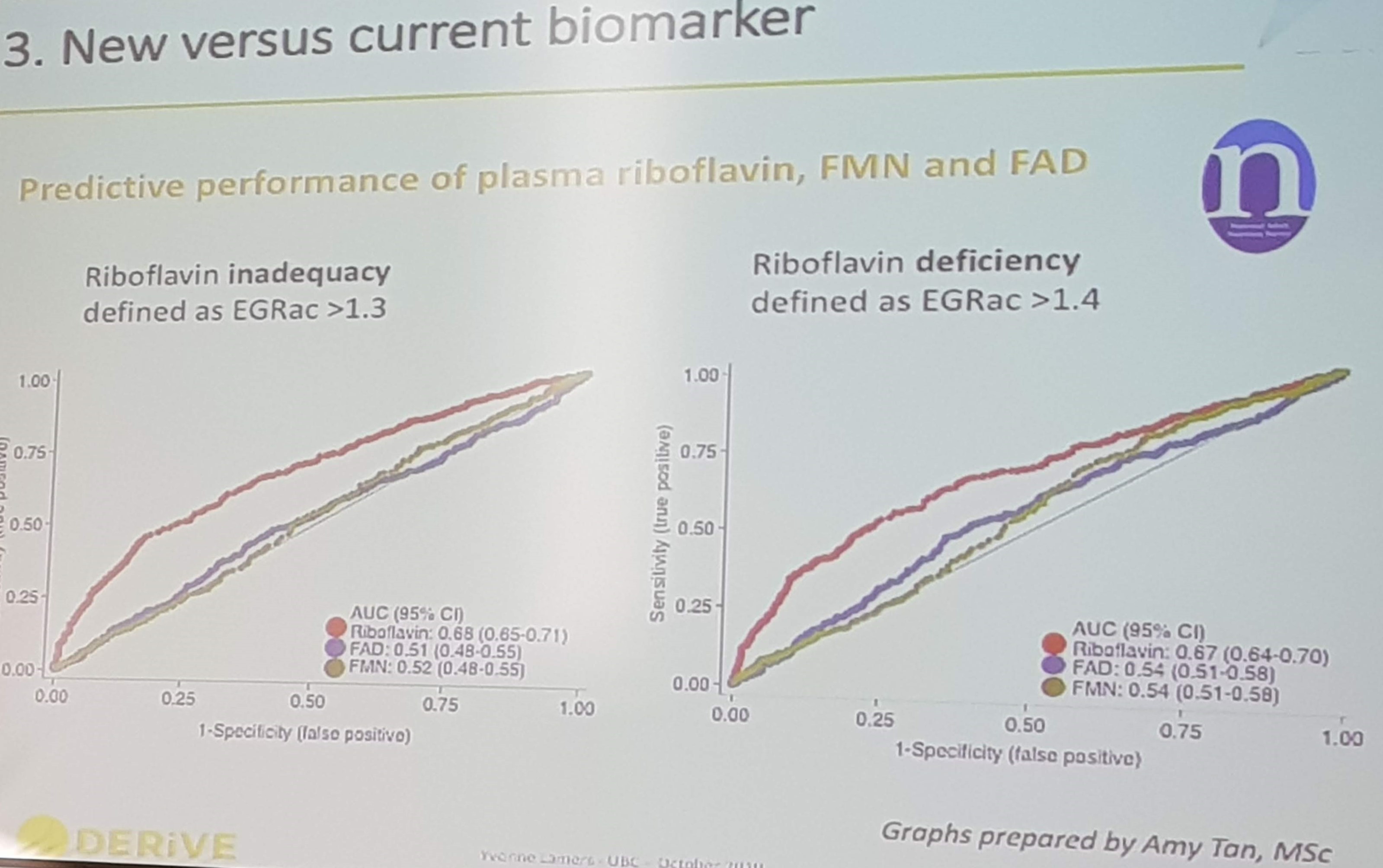
After the session on sweeteners, I made it to the last talk in the session focusing on the DERiVE project, by Yvonne Lamers. She presented data demonstrating that plasma concentrations of the riboflavin markers FAD and FMN are not good markers to predict vitamin B2 status. However, combining FMN, FAD and riboflavin into total plasma riboflavin showed promise as a vitamin B2 status marker, when compared to the gold standard functional marker EGRac (Eryhrocyte Glutathione Reductase activity coefficient).
Credibility vs clickbait
The next step after doing research in nutrition is to communicate the findings to the public. In a session organized by Eat Well Global, this was the topic. Today social media plays a central role in the dissemination of nutrition information, and not always in a good way. Influencers are spreading misinformation at the speed of light, and a big challenge is to
The first speaker was Taylor Wallace, with his thoughts on scientific communication. He emphasized the importance of identifying stakeholders who have the power to implement your message. Preaching to the choir is not an effective way of getting your message across, but is most often what happens in nutrition communication. Further, Wallace emphasized the importance of framing your findings to get your main messages across, and encouraged the use of digital, social and traditional media to disseminate your findings. Non-traditional sources can also be an effective arena for communication, as you could reach audiences you normally wouldn’t reach. Wallace himself appears on the Dr.Oz show, and have published articles on his blog.
The second speaker was Jovanka Vis, who talked about how to use social media to spread science. She started her talk by talking about the echo chamber known as the internet, where everyone has an opinion. She focused on how to frame your message in a positive way, e.g. “eat less meat” vs “there is more than meat”, where the same message is delivered in different packages by changing the focus. Vis showed several example of how the Netherlands Nutrition Centre have communicated their dietary advice to the consumers, using videos, games and being visible in social media. At the end of her talk, Vis encouraged the audience to engage in the debate, and always respond when approached in social media. Never waste a good crisis!
Thursday - Day 3
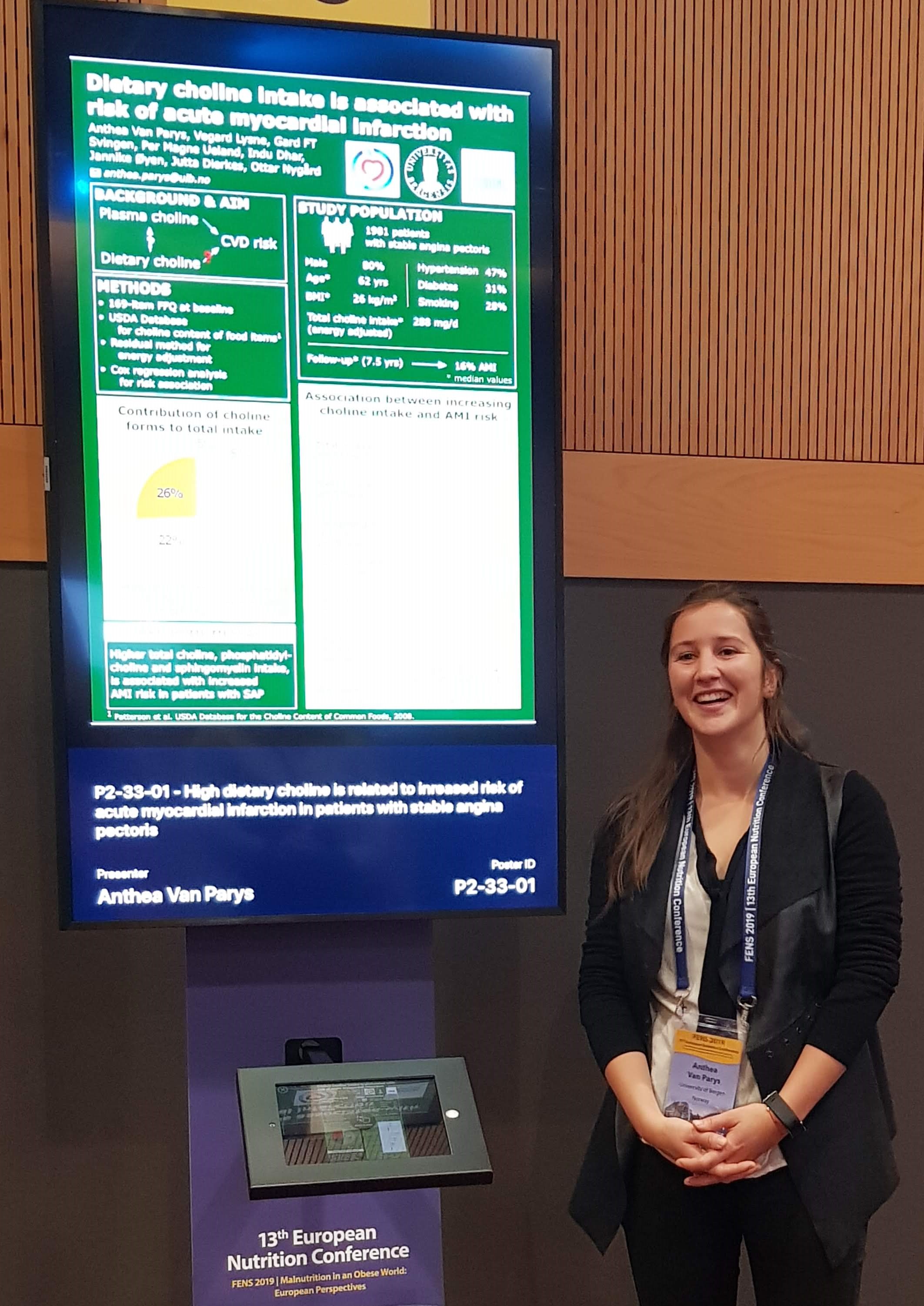
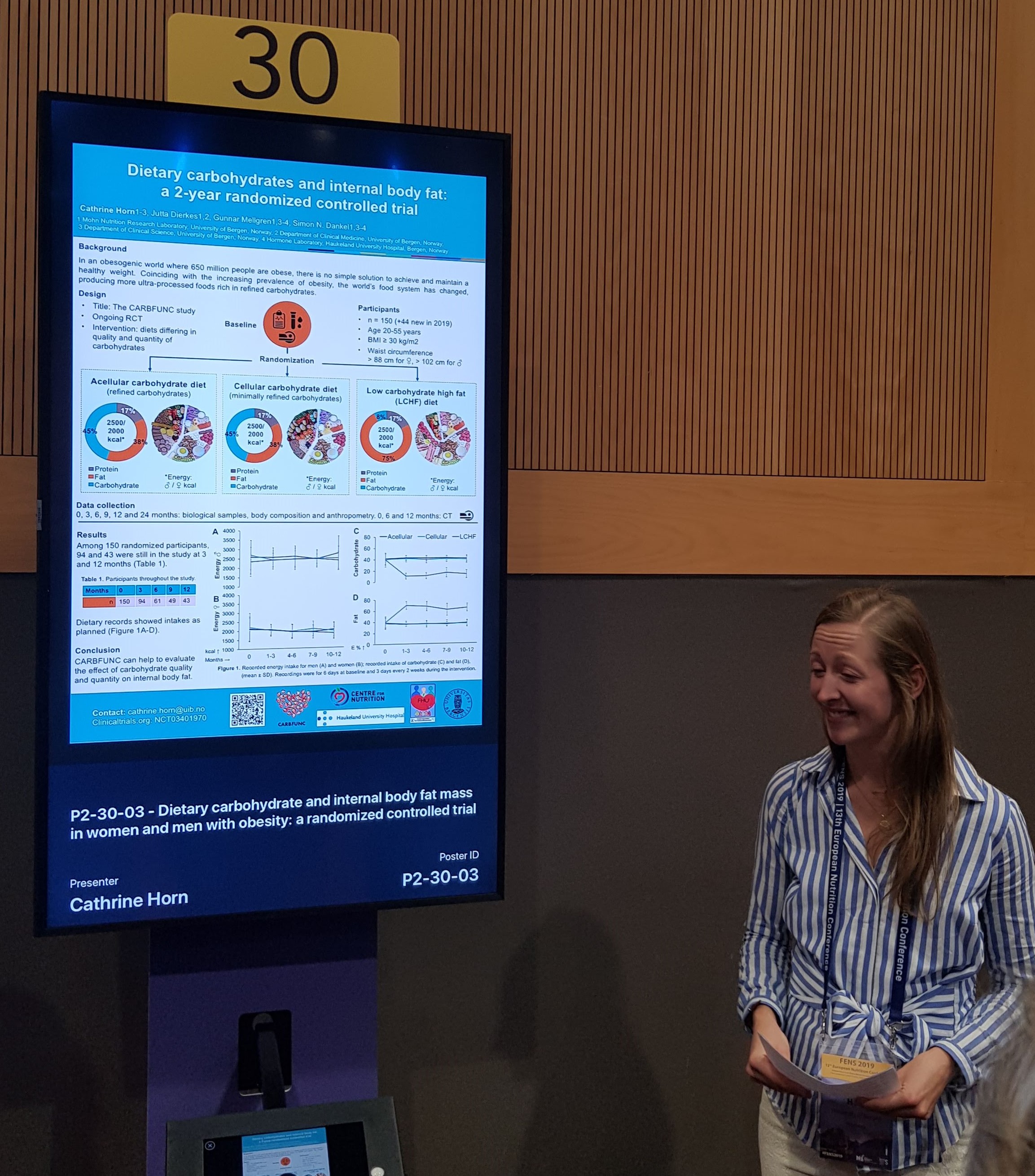
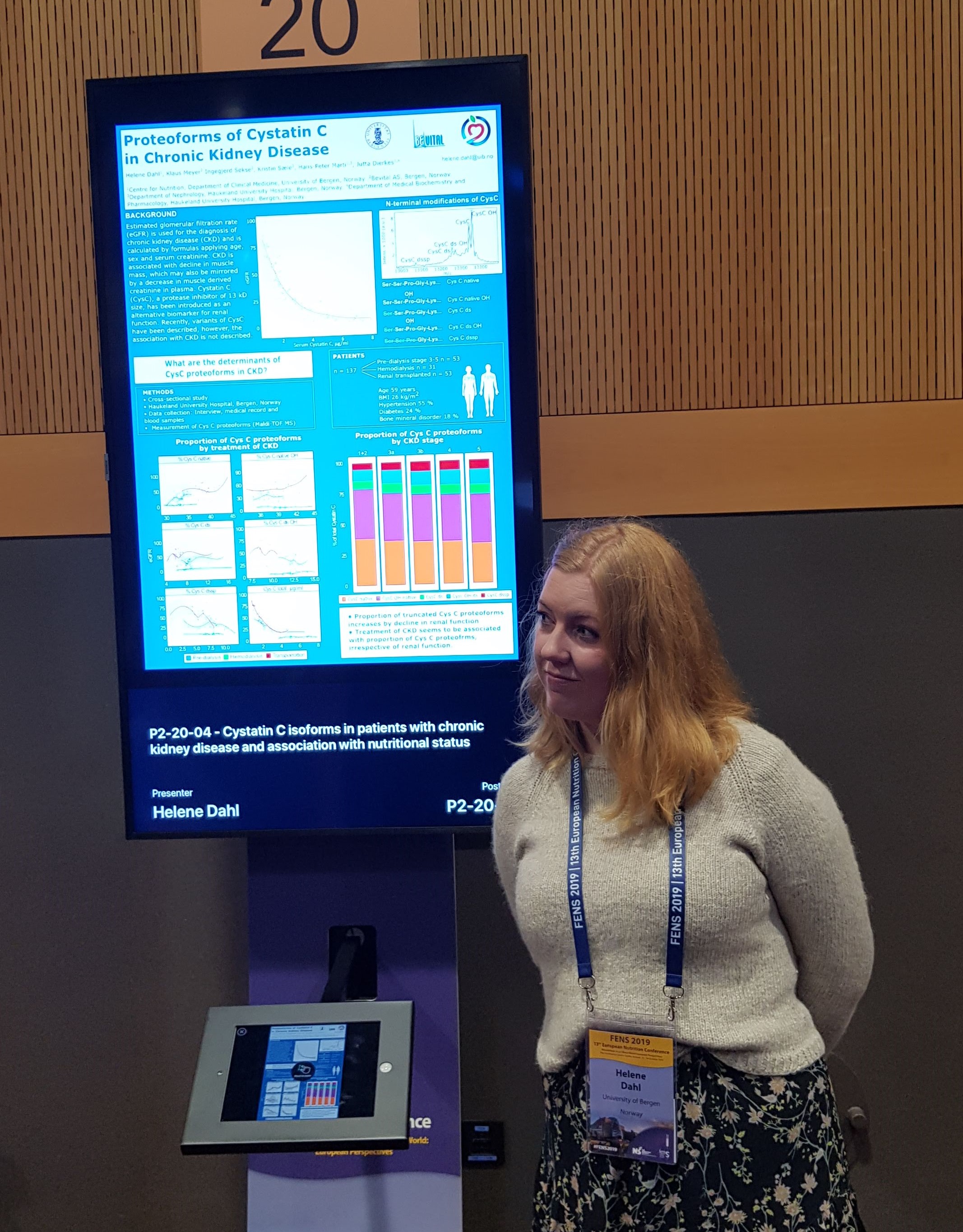
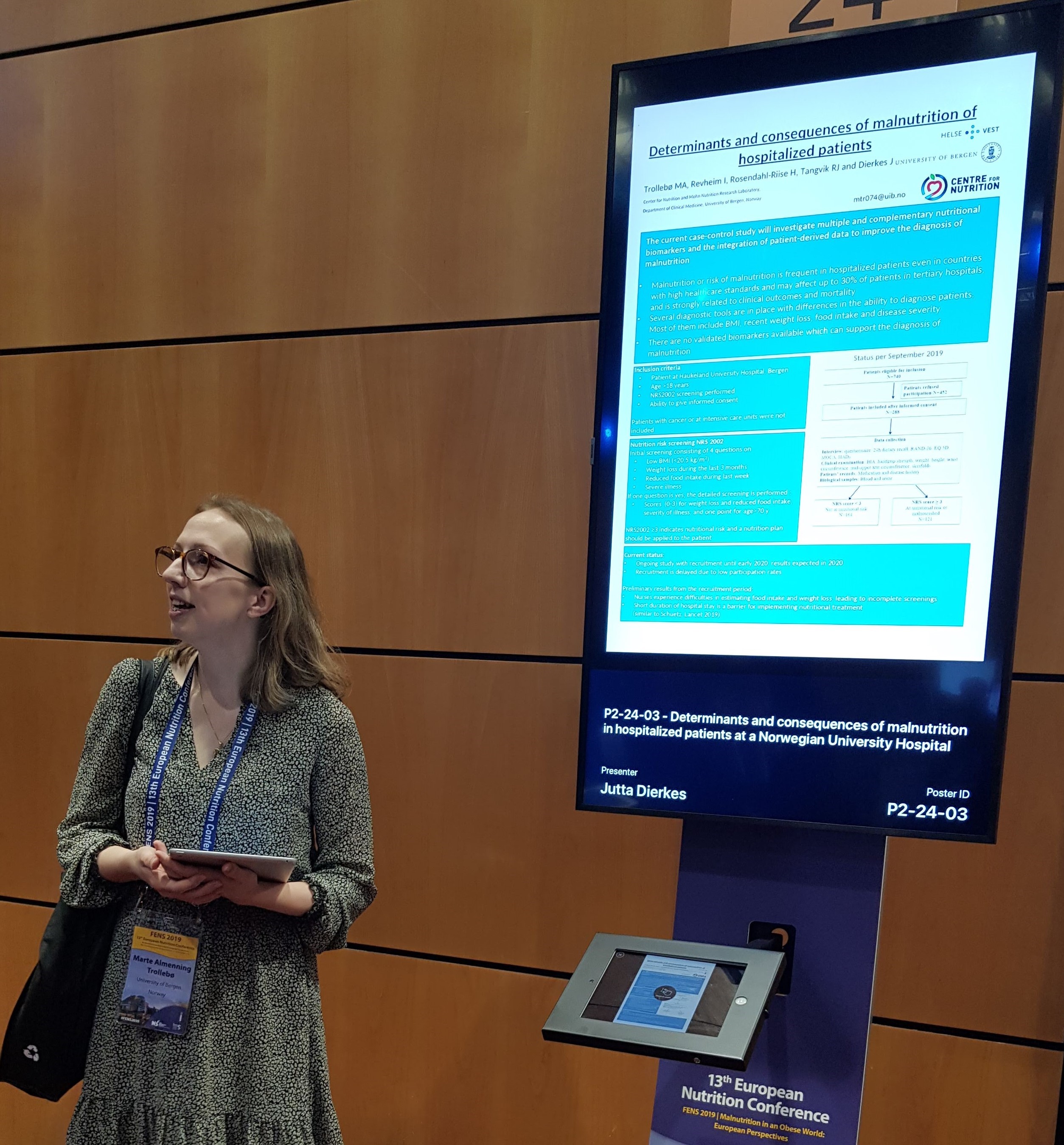
This day started at the poster session, where several of my colleagues, Anthea Van Parys, Cathrine Horn, Marte Trollebø and Helene Dahl, presented their work.
Malnutrition in Obesity
The first plenary session of the day was presented by Ellen Blaak with her talk Current metabolic perspectives on malnutrition in obesity. She started by defining malnutrition, which is not just restricted to deficiency, but any abnormal physiological condition caused by inadequate, unbalanced or excessive intakes. Increasing evidence is suggesting insulin resistance as a parameter to identify subgroups for precision nutrition, but Blaak asked the question if tissue-specific insulin resistance may elicit different metabolic consequences, depending on which tissue is affected.
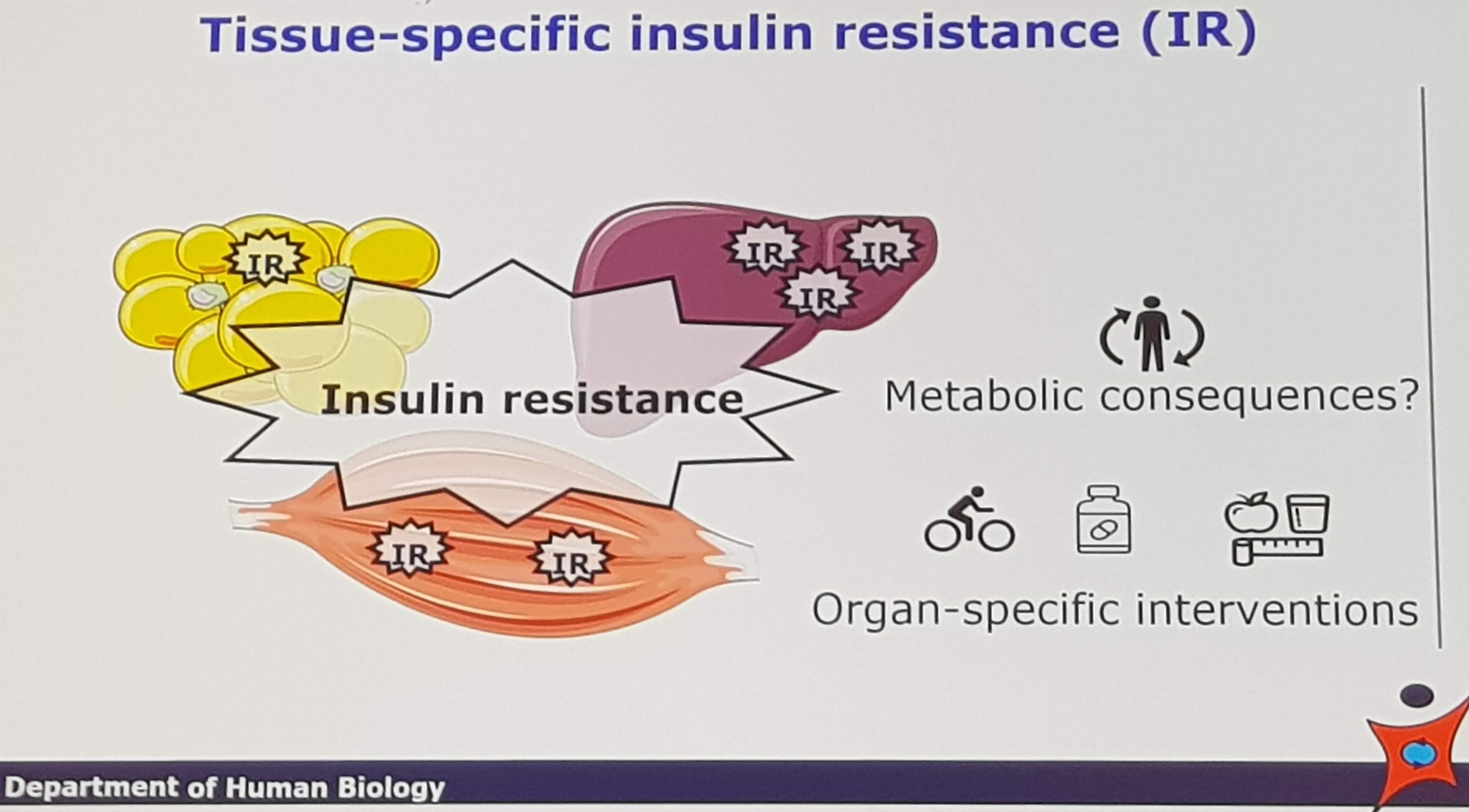 Blaak showed us data investigating metabolomic profiles associated with insulin resistance in the liver and muscle, respectively. Although there were some overlap, there were also some tissue-specific differences. Further, a gender specific effect on plasma lipid profile were observed, where insulin resistance in the liver causes a particular worsening of lipid profile in women. She ended her talk by emphasizing that targeted approaches are needed to optimize nutrition for cardiometabolic health.
Blaak showed us data investigating metabolomic profiles associated with insulin resistance in the liver and muscle, respectively. Although there were some overlap, there were also some tissue-specific differences. Further, a gender specific effect on plasma lipid profile were observed, where insulin resistance in the liver causes a particular worsening of lipid profile in women. She ended her talk by emphasizing that targeted approaches are needed to optimize nutrition for cardiometabolic health.
Ultra-processed food
The next session I attended was on the topic of ultra-processed food. This is a concept I’m personally struggling with. I get the overall point that highly processed food on average is often not the most healthy options. My main problem is that I cannot find a simple definition of what ultra-processed foods are, and as there are also many good aspects of food processing I’m not sure if this is a good way of categorizing what is healthy and what is not. I’m not convinced that such a system is needed to identify healthy foods in general. However, this may perfectly reflect my own ignorance, and I hope this session will convince me that I’m wrong!
The first talk was by Jean-Claude Moubarac, trying to provide an overview of what ultraprocessed foods are and how they influence overall dietary processing. He started by giving an overview of the evolution of food processing, and pointed out that we’re no longer working with ingredients, but with molecules.
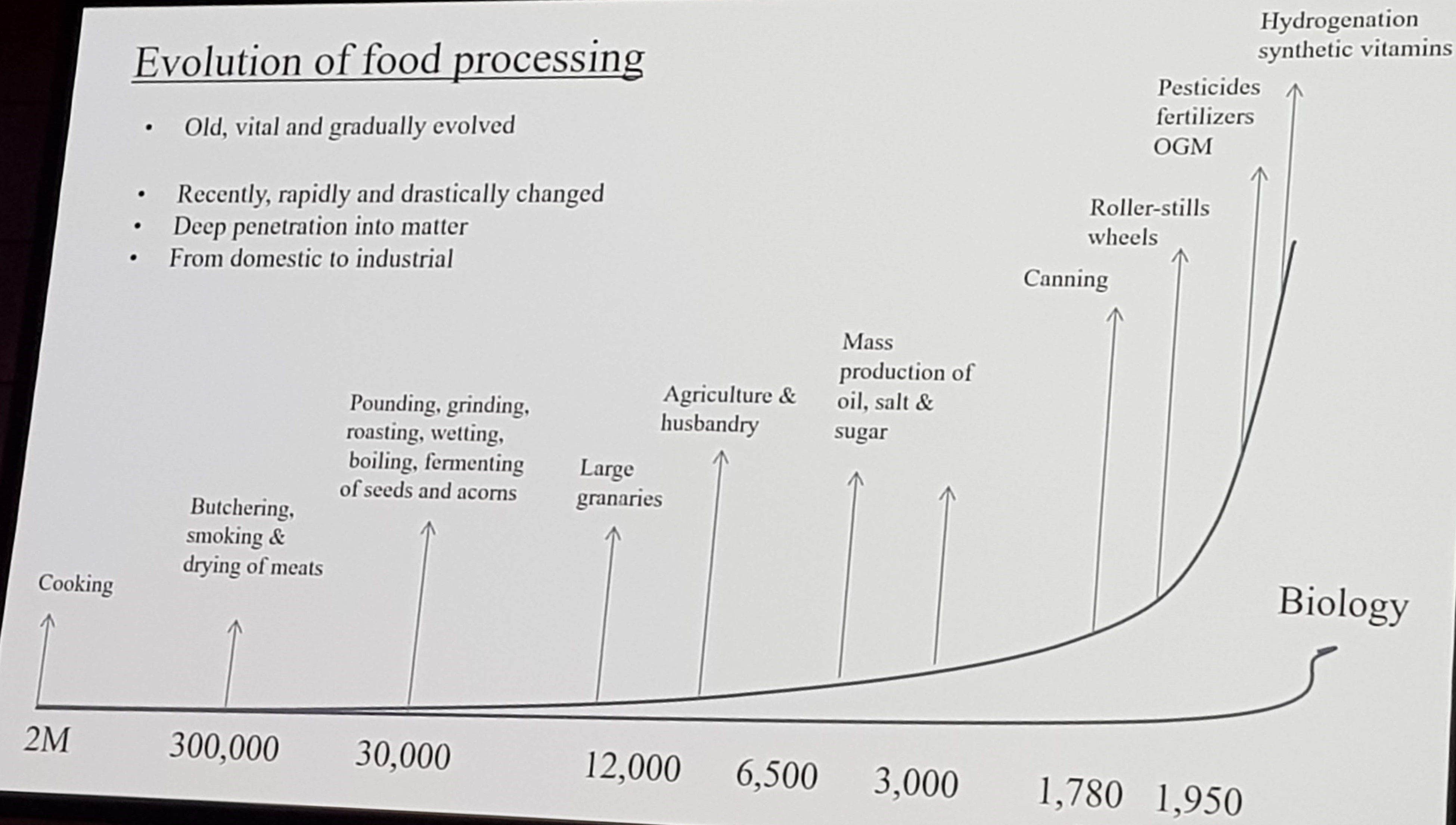 He further introduced the NOVA classification. The first group includes unprocessed or minimally processed food. The second group includes processed culinary ingredients such as sugar and oils. Group 3 include processed foods, such as cured meat. The last group is the ultraprocessed foods, which is industrial foods and drink formulations made mostly from refined artificial substances and additives. Consumption data demonstrate that the intake of foods from the NOVA group 4 is increasing at a rapid pace, and there are concerns regarding how this influence the overall quality of the diet.
He further introduced the NOVA classification. The first group includes unprocessed or minimally processed food. The second group includes processed culinary ingredients such as sugar and oils. Group 3 include processed foods, such as cured meat. The last group is the ultraprocessed foods, which is industrial foods and drink formulations made mostly from refined artificial substances and additives. Consumption data demonstrate that the intake of foods from the NOVA group 4 is increasing at a rapid pace, and there are concerns regarding how this influence the overall quality of the diet.
Data from the NOVA multi-country study shows that those with the highest intake of ultraprocessed foods eat more energy, more added sugar, more salt, less fiber, less protein and less micronutrients. In general, higher consumption of nutrients we want to limit, and lower consumptions of favorable nutrients. A healthy diet is low in ultra-processed foods.
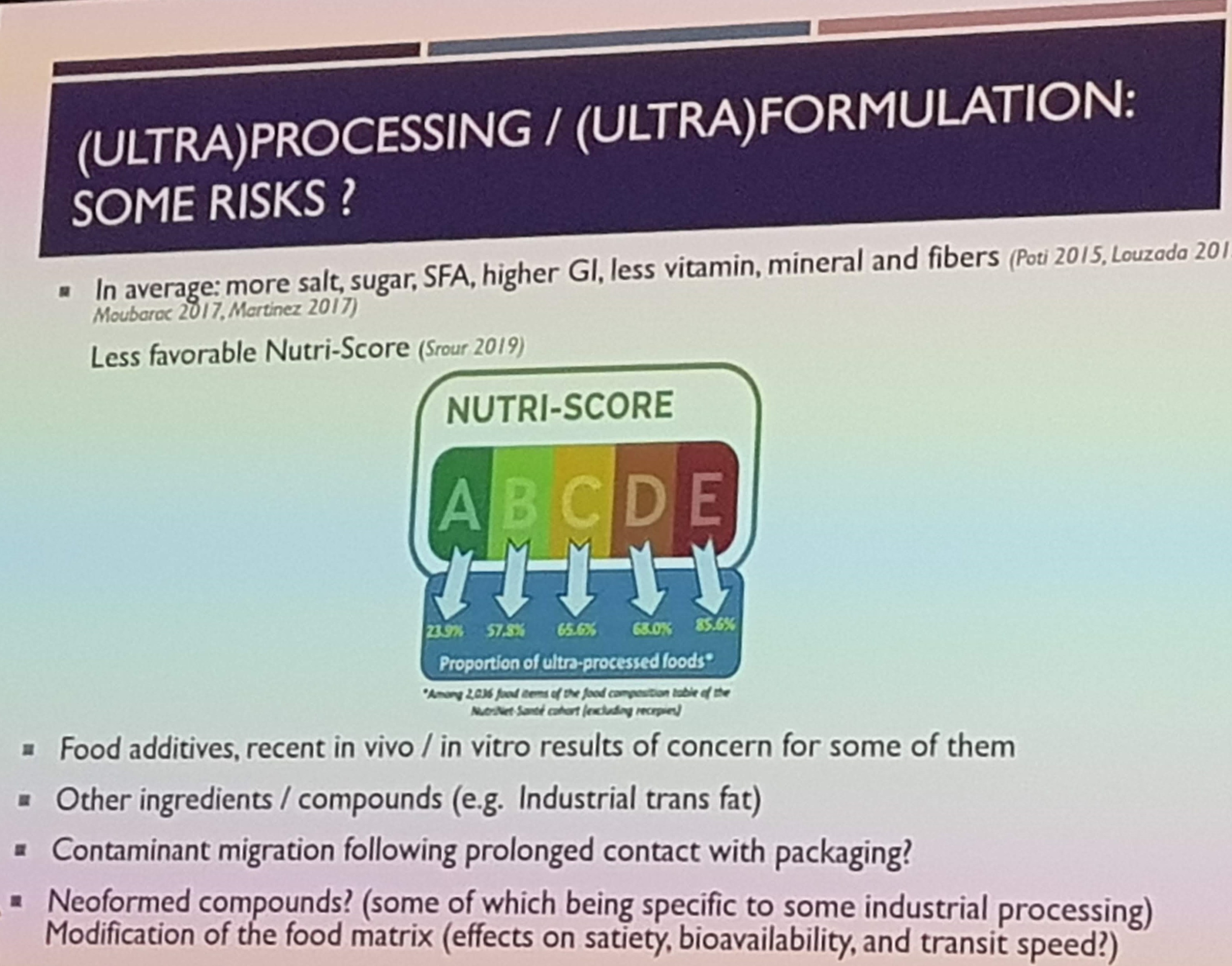
The symposia was continued with a talk from Mathilde Touvier, presenting epidemiological perspectives on ultra-processed foods and health. She started by underlining the good sides of food processing, in terms of reducing microbiological risk, increasing bioavailability and increasing shelf-life. She introduced the NUTRI-SCORE, a scale from A-E classifying the nutritional quality of foods. In the E category, 85% of the foods are ultra-processed. However, 24% of the foods in the A category is also ultra-processed, and 60-70% of the B-D categories. This suggests that not all ultra-processed foods are alike when considering nutritional quality.
 In the NutriNet-Santé cohort, ultra-processed foods comprises 18 % of the food intake, but contributes with 35% of the energy intake. Further, higher intake of ultra-processed foods are associated with increased risk of cancer, cardiovascular disease, diabetes and mortality. When performing similar analyses for unprocessed food intakes, they observed lower risk.
In the NutriNet-Santé cohort, ultra-processed foods comprises 18 % of the food intake, but contributes with 35% of the energy intake. Further, higher intake of ultra-processed foods are associated with increased risk of cancer, cardiovascular disease, diabetes and mortality. When performing similar analyses for unprocessed food intakes, they observed lower risk.
The final talk of the session was given by Marit Kolby Zinöcker, with her presentation on potential Mechanisms connecting Ultra-processed Foods with Gut Inflammation. She started by stating the obvious: unhealthy diets are drivers of metabolic disease. The question is how, and Zinöckers hypothesis is that changes introduced during food processing causes low-grade inflammation by interacting with the microbiome. She introduced the concept of acellular foods/nutrients. Normally, nutrients are contained within the cell structures, but during processing these structures are broken down. This makes the nutrients more available in the small intestine, increasing the potential for bacterial growth. Further, less nutrients is transferred to the microbiota in the colon. Altogether, according to her hypothesis, this may cause low-grade inflammation. Zinöcker concluded her talk by saying that when the jury on these foods are out, we should probably emphasize eating more freshly made foods and less highly processed foods. I think we all agree with that conclusion regardless of our stance on the concept of ultra-processed foods.
Food environments and the obesity epidemic
Nicely following the session on ultra-processed food, the next plenary session, presented by Lauren Lissner, was on the topic of food environment and the obesity epidemic.
Lissner first defined the food environment as consisting of political, socioeconomic, and physical factors that affect accessibility and healthfulness of diets, and some of these aspects are relevant for the development and prevention of obesity. One aspect is the quality of the foods we eat, with concepts such as ultra-processed foods. A recent review concluded that a minority of packaged foods could be considered healthy. Intervention studies also shows that when eating ultra-processed foods, the energy intake on average is higher. One possible mechanisms can be related to increased eating speed. One problem that was pointed out is the fact that in some areas, the “food deserts”, we not only face the situation of too few healthy options, but also the challenge of too many unhealthy options.
Lissner continued her talk by focusing on obesity in children. She presented data from a study observing that children with a taste preference of high-sugar or high-fat foods were more likely to be overweight. Further, socio-cultural aspects such as eating while watching TV, is related to increased risk of overweight.
The talk was finished with some perspectives on political factors. One such aspect is front-of-package labels such as the key hole or the NUTRI-SCORE. These labels are more easily accessible to the consumer compared to the traditional back-of-package labels with information on nutrient content and ingrediences. These labels also provide an incentive to challenge the industry to reformulate their products to qualify for these labels. Another political aspect is the promotion of plant-based diets for environmental reasons. Are these diets less obesogenic? A recent study observed that those increasing their intake of plant foods were more likely to lose weight, while those increasing their intake of meat were more likely to gain weight. Lissner emphasized that in addition to health effect, future nutrition policy must also take into account other effects of diet, such as environmental impact.
Health effect of individual fatty acids
The first talk was gived by Philip Calder, presenting a systematic review of the effects of increasing arachidonic acid intake. Arachidonic acid (AA) is an omega-6 polyunsaturated fatty acid primarily found in meat, organ meats and eggs. Albeit AA make up a small part of total fat intake, it makes up a substantial proportion of the fatty acids in different tissues. AA is a substrate for many lipid-derived signaling molecules, and many common drugs such as aspirin is working by interfering with these pathways.
Increasing AA intake lead to increased AA incorporation in tissues. However, no particular effects on clinical parameters such as lipid profile, blood pressure and inflammation. However, one study suggested a protective effect against age-related cognitive decline, and there are data suggesting benefits in regard to physical performance, especially increasing peak anaerobic power with high doses. In summary, there are no reported harmful effects of increasing AA intake to much higher levels than current intakes. On the other hand, the effects of lowering intakes are not known.
The next talk of the session was presented by Ronald Mensink, giving an update on the hot topic of potential health effect of omega-3/6 intakes and balance. His talk started by reiterating that there are only two essential fatty acids, linoleic acid (LA, omega-6), found in nuts, sunflower oil and soybean oil, and alphalinoleic acid (ALA, omega-3), found in nuts, rapeseed oil and flaxseed oil. These fatty acids are converted to the longer polyunsaturated fatty acids. Mensink talked us through what we know about the effect of these different fatty acids, and how they interact.
A common topic is the ratio between LA and ALA in the diet. However, Mensink pointed out that this ratio does not predict the conversion to the longer fatty acids, which is entirely driven by the absolute amount. Also when including other omega-3 and -6 fatty acids, changes in this ratio can reflect changes in one, the ohter or both. Mensink concluded that this ratio is not useful to predict the healthiness of a diet. The talk was closed with the statement that a universal marker of fatty acid intake would be nice to have, but is unlikely to exist.
Peter Joris closed the session with a talk considering the health effects of different saturated fatty acids. He opened with talking through the well established effects of substitutions between different nutrients, where the most beneficial metabolic profile is observed when replacing saturated with polyunsaturated fatty acids. However, less focus has been given to the effect of specific saturated fatty acids. We know that different saturated fatty acids have different effects on the lipid profile, and different associations with disease risk has also been reported. Further, short- and medium chained fatty acids elicit different effects on energy metabolism compared to long-chained fatty acids.
Joris and colleagues are currently working on a systematic review, focusing on how the individual saturated fatty acids impact traditional risk markers as well as disease risk. The review will also take into account factors such as food matrix effects.
Nutrition sciences beyond reductionism
For the final session of the day I decided to attend the session on nutrition sciences beyond reductionism. The benefits of nutrition interventions aiming at prevention of chronic diseases can most often not be related to one single cause. Reductionist approaches does not work, but are still widely used. The main focus of this workshop was what we as nutrition researchers can do to improve the quality and credibility of our field.
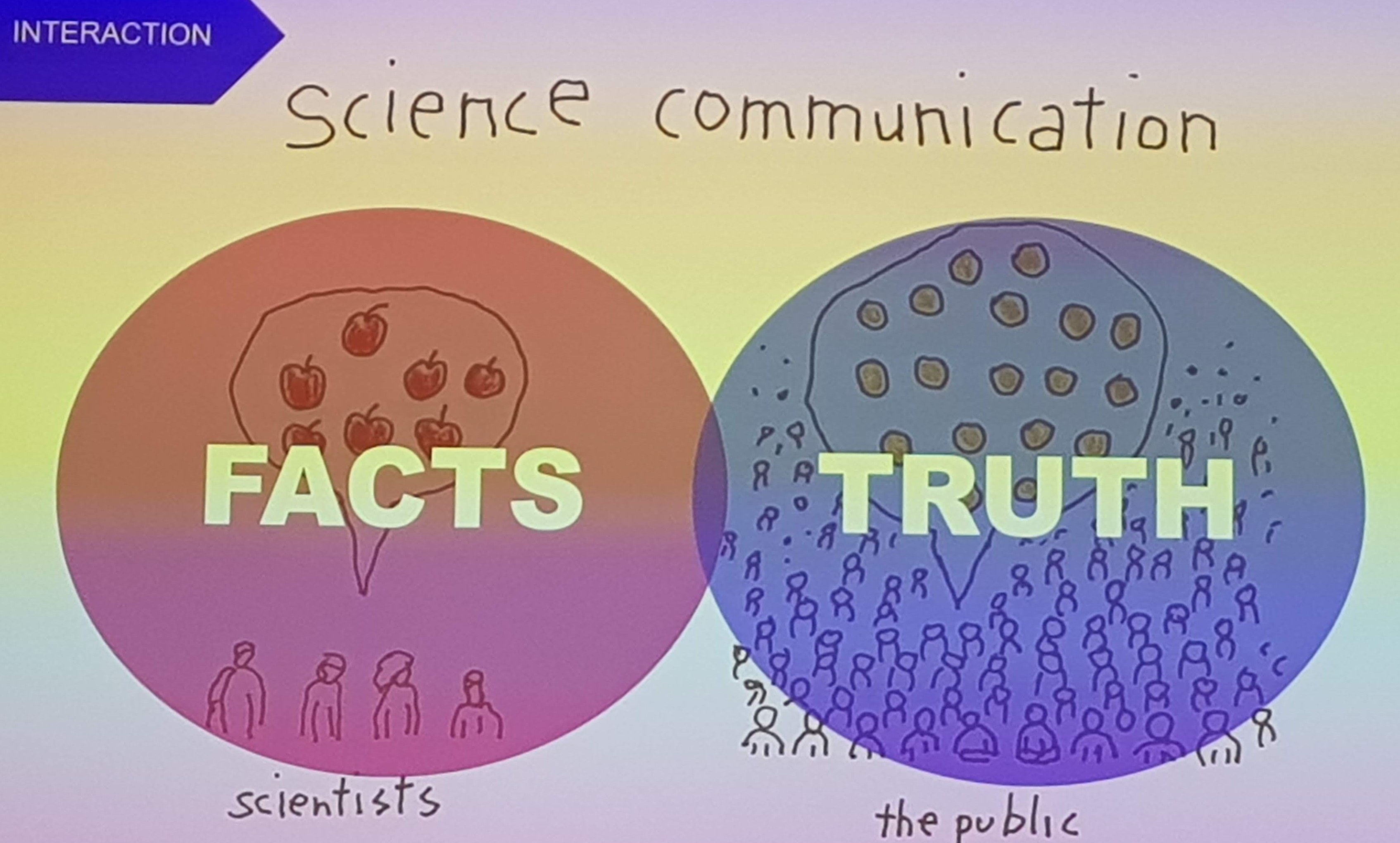
First, Edith Feskens presented a talk on The concepts in Nutrition in Transition, introducing the overall focus of the initiative. The first concept was related to how we look at evidence. Is the time up for the evidence pyramid, and should it be replaced by other approaches more suitable to the nutrition field? The other concept was related to mechanistic insights, which is based on evidence low in the evidence pyramid, but also play an important role in our overall understanding. The third concept was related to funding and organization. We are often dependent on private funding, but is this influencing the content and credibility of the overall message which is communicated to the public? The final concept related to science communication. What scientists are communicating is only a small part of what is eventually perceived as truth.
Next up, Pieter van het Veer summarised the Result of discussion from the Satellite “Nutrition in Transition”. He started his talk by providing the FAO definition of healthy and sustainable diets, which combines biomedical, cultural and ecological perspectives. The question is whether nutrition research is really fit for the 21st century diet. Some of the challenges is related to implementing research on multiple levels, including personal and the system, as well as including inter-generational effects including sustainability. Currently we are focused on studying the relationship between diet and health outcomes, but should also start thinking about other domains, such as food intake being an outcome of the food environment and consumer behaviour. Further, more focus should be put on science communication to put the science in context, both upstream to policy makers, and downstream to consumers.
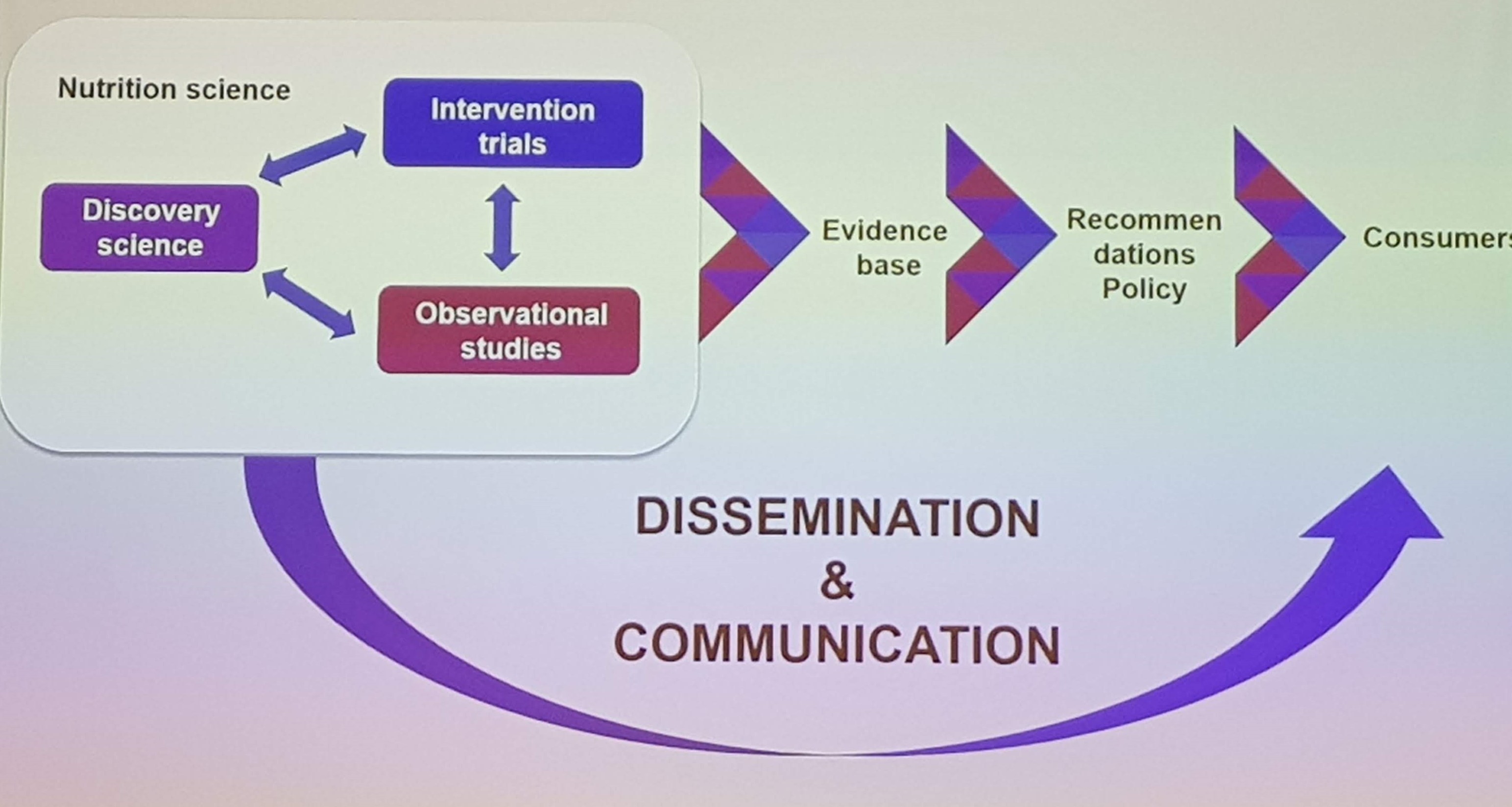
The next talk was delivered by Philip Calder, on Ensuring Trust in Nutrition Science. The core of nutrition science is made up of a combination of observational, interventional and mechanistical work, which make up the evidence base underlying recommendations and nutrition policy. He pointed out that recommendations often focus heavily on the interventional studies, which in humans are very hard to do, and ignore other lines of evidence which also contribute to what we know. Robust recommendations should be based on the whole evidence base, acknowledging its strenghts and limitations.
 Another key point is communicating this to the public, and Calder underlines that the communication of nutrition research to the public is poor. This leads to public confusion, distrust, lack of care, and eventually people starts getting their advice from poorly informed “experts”.
Another key point is communicating this to the public, and Calder underlines that the communication of nutrition research to the public is poor. This leads to public confusion, distrust, lack of care, and eventually people starts getting their advice from poorly informed “experts”.
Friday - Day 4
You are when you eat
On the last day of the conference, after a late night out, I attended the session on chrononutrition. More focus has been given to not only what we eat, but when we eat, making this a hot topic in nutrition today.
The opening talk was given by Gerda Pot, Chrono-nutrition: epidemiological evidence of meal timing on health. She started by defining chrononutrition as the relationship between diet and biological clock, including when you eat, how frequent you eat and how (ir)regular you eat. When considering when we eat, there are data showing that the same dietary intake at different times elicit different effects, and especially that eating late is associated with increased body weight. Further, irregular meal patterns has been consistently linked to increased risk of obesity and metabolic syndrome. The data on meal frequency is mixed, but overall it seems to have little impact. She further presented some preliminary data from the SUSPend study, comparing adolescents with biological clock disorder with controls, and so far this was associated with more irregular meal patterns, later dietary intake, and higher body weight.
Next up, Jonathan Johnston gave a talk on how meal timing influences circadian rhythm. He provided a definition of the term circadian as referring to endogenous rhythms, purely driven by biology. To keep our biological clocks aligned with the world, they are synchronized by different factors, zeitgebers, of which light exposure by far is the most studies. Johnston presented data showing how gene expression varied throughout the day, involved in glucose and lipid metabolism. In a study investigating the effect of meal timing, they demonstrated that delaying food intake had a powerful effect on glucose metabolism, but didn’t impact the triglyceride rhythms. However, eating at different times did elicit different postprandial responses, with larger increases in blood sugar when eating later in the day. At the end of the talk, a pilot study on time-restricted feeding was presented. By delaying the first meal and moving the last meal forward, the main effect was seen for energy intake which was lower when shortening the eating window.
The final talk of the session was given by David Bechtold, on the Recipricol connections between the timing of food intake and the circadian clock. He pointed out that rhythmic feeding was one of the major determinants of the biological clocks, and presented molecular data on how the clocks may respond to meal timing. In a recent study they demonstrated that insulin treatment was able to modulate the biological clocks, suggesting that food intake can influence the clocks via insulin signaling. However, the main question is whether it matters if diet influences circadian rhythms. Using data from animal studies, Bechtold argued that alterations in the biological clocks may disrupt the metabolic adaptation to both low and high energy intakes.
Epigenetic reprogramming
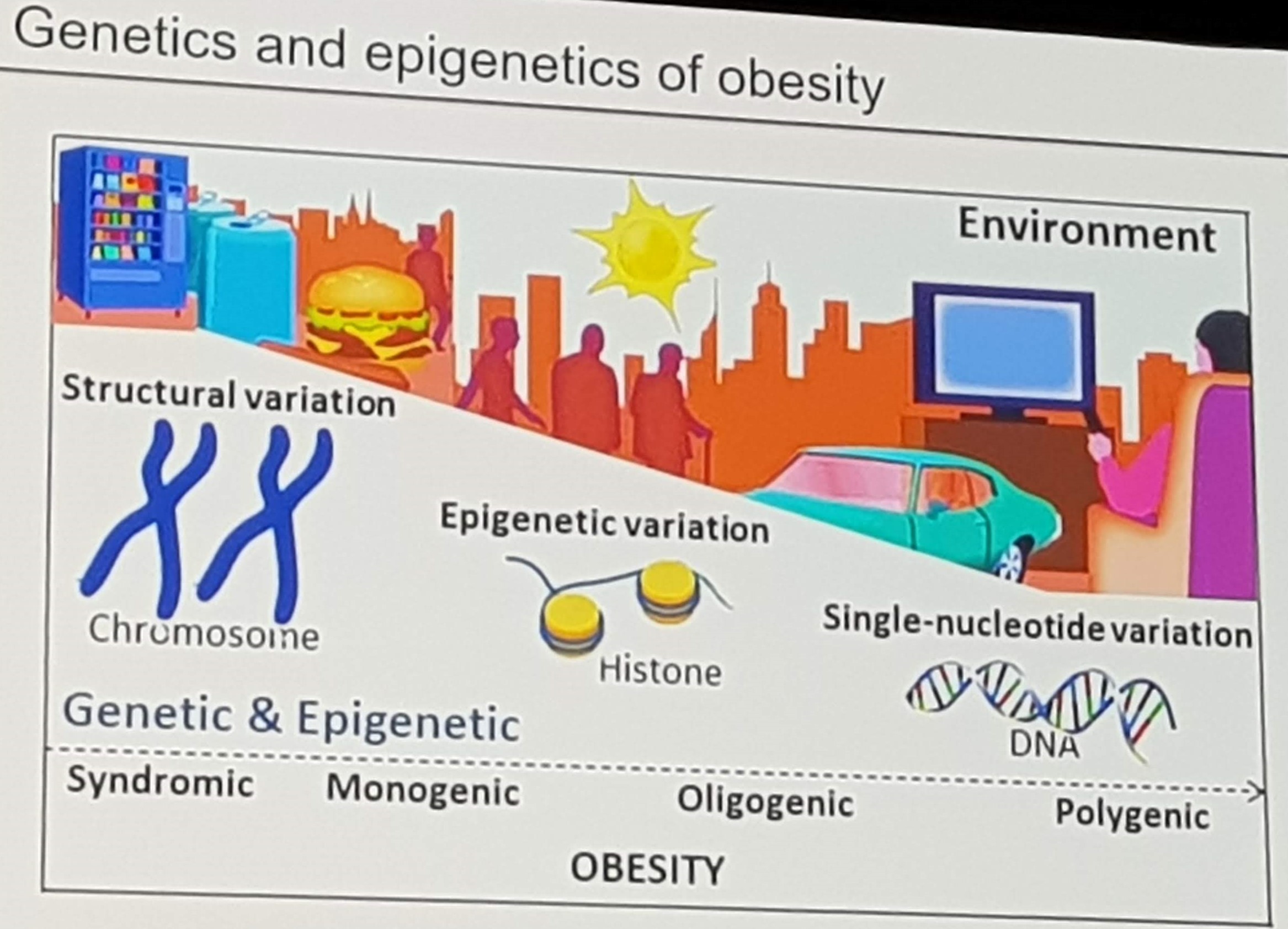
The final session of the conference was a plenary session on epigenetic reprogramming, presented by Christian Wolfrum. His focus was on the heritability of obesity, which cannot be explained by genetics alone.
 There are several studies suggesting that maternal dietary intake and abnormal weight gain during pregnancy increases the risk of obesity in the next generation. However, mechanistic studies in animals are mixed, suggesting that the heritability may also be a question of social imprinting where obesogenic habits are transferred to the child.
There are several studies suggesting that maternal dietary intake and abnormal weight gain during pregnancy increases the risk of obesity in the next generation. However, mechanistic studies in animals are mixed, suggesting that the heritability may also be a question of social imprinting where obesogenic habits are transferred to the child.
The second part of the talk was devoted to brown fat, which increases energy expenditure through heat production. Brown fat is known to be activated by cold temperatures, but recent evidence also suggests that people born in the coldest part of the year have more brown fat compared to those born in the summer.
And that concluded the FENS conference 2019. In 4 years, the conference will be arranged in Serbia, and in the mean time I hope to attend the Nordic Nutrition Conference 2020 in Finland, and the International Congress of Nutrition 2021 in Tokyo.